Ringworm fungal infections are common in the US and are becoming increasingly resistant to treatment – 6 questions answered
The World Health Organization considers antimicrobial resistance to be one of the most serious threats for global health. Similar to the way bacteria have developed resistance to antibiotics, fungal infections throughout the world are becoming more drug-resistant and more deadly.
In early 2023, the New York State Department of Health reported two cases of severe tinea, a contagious type of ringworm infection. The Centers for Disease Control and Prevention later reported that they were caused by a species of fungus that has been spreading throughout South Asia over the past decade.
The Conversation spoke with Rodney Rohde, a medical laboratory professional and public health microbiologist, about the prevalence of ringworm and the growing threat of antifungal resistance around the world.
1. What is ringworm and how common is it?
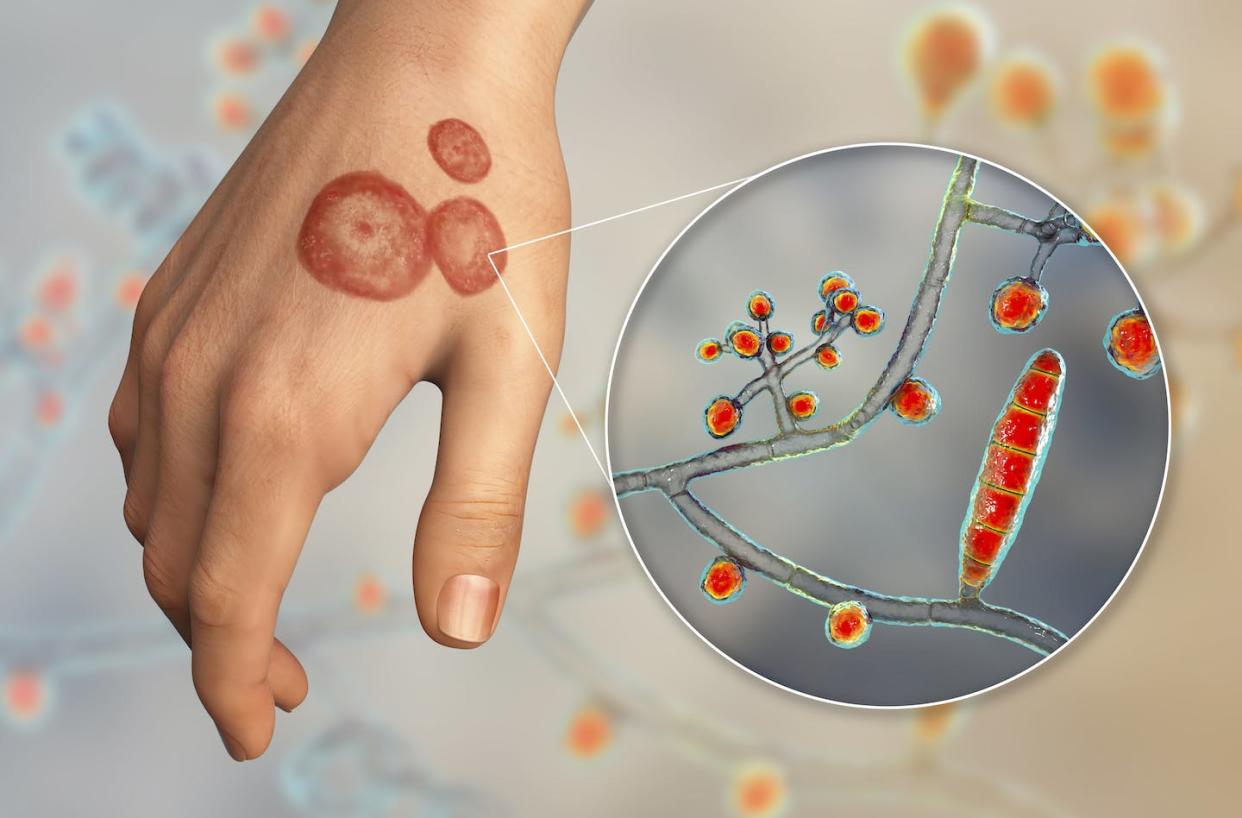
When one hears the term ringworm, it likely conjures images of a nasty parasitic worm infection. However, a ringworm infection is a common infection of the skin caused by a fungus. Experts state that about 20%-25% of the population will experience a ringworm infection at any given time.
Fungi can be found almost anywhere – soil, plants, surfaces, on the skin and in our bodies, and even in the air. Research shows that there are up to 40 types of fungus that can cause these ringworm infections, with the most common types being from the genuses Trichophyton, Microsporum or Epidermophyton.
Medical terms for ringworm are “tinea” and “dermatophytosis.” Tinea and dermatophytosis are synonyms for a contagious fungal infection of the skin. Other names for ringworm are based on its location on the body – for example, ringworm on the feet is commonly called athlete’s foot, and ringworm associated with the groin area is referred to as jock itch. These are characterized by a persistent itchy rash that can appear flaky and cracked.
While anyone can be infected, ringworm is most commonly picked up in the following circumstances:
– A weakened immune system or an autoimmune disease like lupus.
– Playing a high-contact sport, like wrestling; this ringworm is called tinea gladiatorum.
– Profuse sweating, also known as hyperhidrosis.
– The use of public showers or locker rooms.
– Handling or working with infected animals.
– Living in a subtropical or tropical region.
2. How can you recognize ringworm?
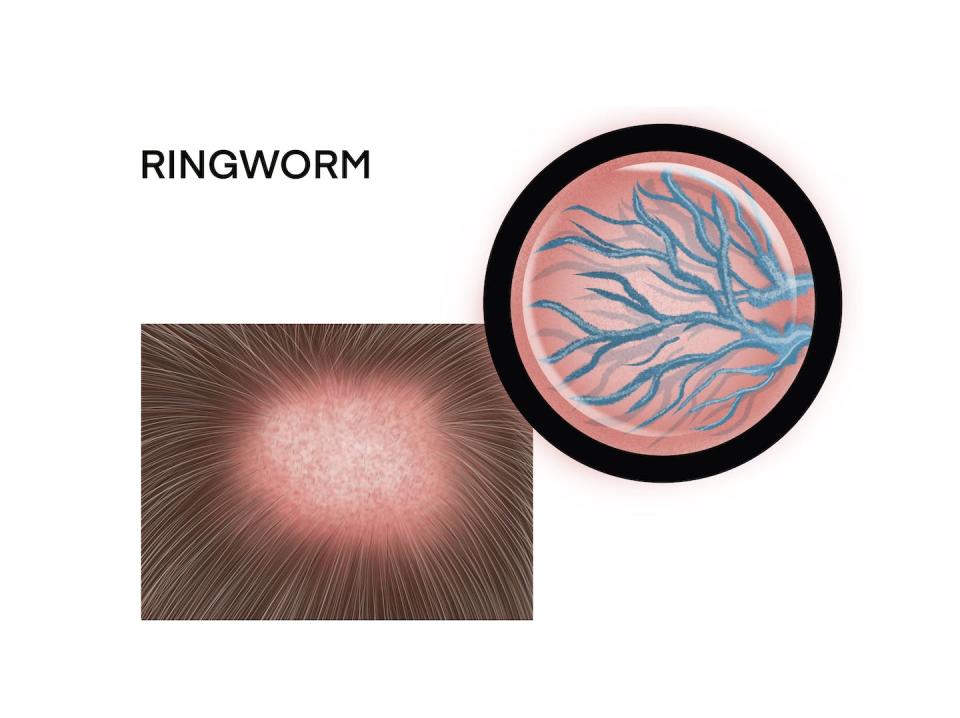
The hair, skin and nails of either fingers or toes are the likely landing spots for a ringworm infection. Signs and symptoms of an infection usually depend on which part of the body is affected, but generally may include hair loss and red, scaly, cracked skin. However, the most well-known sign that gives this infection its ironic and misplaced name – ringworm – is the hallmark ring-shaped rash.
3. How does ringworm spread?
Many fungi can be seen with the naked eye, such as common mushrooms or bread mold.
Fungi can grow in two forms: yeasts, which are single round cells, and molds, which are made up of many cells forming long, thin, hairlike threads called hyphae. Some of them can exhibit both forms of growth and thrive in decaying organic material like soil or a plant. But fungi can also grow in unexpected places, such as on wallpaper.
Fungi are relatively easily transmitted because of their ability to survive on a diversity of surfaces, including medical devices.
Fungal transmission occurs via three primary routes: by coming into close contact with another person who has a ringworm infection; by touching an infected animal, be it livestock, pets or wildlife; or by contacting an infected surface.
Some types of fungi can thrive where it’s warm and humid. Ringworm occurs more frequently in tropical areas and during hot, humid summers.
4. How can you reduce the likelihood of getting it?
Some of the best ways to reduce or prevent a ringworm or other fungal infection include:
– Wash hands with soap and warm water.
– Have your pets checked regularly for ringworm.
– Wear shoes and socks that are made of lightweight, breathable materials to reduce moisture.
– Avoid walking barefoot in wet or humid areas like locker rooms or public showers.
– Clip fingernails and toenails regularly to keep them short and clean.
– Change socks and underwear at least once a day, since bacteria and fungi like most, humid environments.
– Avoid sharing clothing, towels, sheets or other personal items with others.
– For athletes involved in close contact sports like wrestling, shower immediately after practice or a match and keep all sports gear and uniform clean.
– Do not share sports gear such as helmets with other players.
5. What treatments are there?
A dermatologist can typically diagnose a ringworm infection visually, but in some cases a small skin scraping, hair or nail sample may be needed for microscopic examination.
There are several treatment options, including antifungal medications prescribed by a physician or dermatologist or over-the-counter products sold as a cream or ointment. A dermatologist may also prescribe an oral pill such as griseofulvin or terbinafine.
Popular over-the-counter products include clotrimazole, sold as Lotrimin or Mycelex, or topical miconazole. For more severe cases, a doctor might prescribe options such as itraconazole medications or tolnaftate.
Finally, in some cases a person may need to use antifungal shampoo and soap to clean themselves and sterilize bedding and clothing.
But treatments don’t always work.
6. Why is antifungal resistance a growing problem?
Antimicrobial resistance, including antifungal resistance, is an ongoing global emergency. Experts estimate that drug-resistant infections caused roughly 1.3 million deaths around the world in 2019. By 2050 that figure could rise to 10 million deaths each year.
Over the past 10 years, South Asia has been experiencing an epidemic of antifungal-resistant ringworm caused by the spread of a novel species of fungus called Trichophyton indotineae, which causes skin disease in both animals and humans. Experts believe that inappropriate use of topical antifungal and corticosteroid medications is likely driving its spread.
In February 2023, a New York City dermatologist reported to public health officials two cases in which unrelated patients with severe tinea caused by Trichophyton indotineae were not improving with oral antifungal treatment. A CDC report found that those were the first cases of tinea from that species in the U.S. One of the two patients had no recent international travel history, suggesting that it could be a case of local transmission of Trichophyton indotineae in the U.S.
This article is republished from The Conversation, an independent nonprofit news site dedicated to sharing ideas from academic experts. The Conversation has a variety of fascinating free newsletters.
It was written by: Rodney E. Rohde, Texas State University.
Read more:
Rodney E. Rohde has received funding from the American Society of Clinical Pathologists, American Society for Clinical Laboratory Science, U.S. Department of Labor (OSHA), and other public and private entities/foundations. Rohde is affiliated with ASCP, ASCLS, ASM, and serves on several scientific advisory boards. See https://rodneyerohde.wp.txstate.edu/service/.